
How to Know When You Are Done with Therapy: A Research-Based Guide to Termination

The ultimate mark of success in my practice isn't how long a patient stays, but how effectively they learn to leave. It's a paradox that often leads to a common question: how to know when you are done with therapy. You've likely spent months or years building a foundation of trust, so the thought of walking away can feel like losing a vital safety net. It's natural to worry about a relapse or feel a sense of guilt about ending a relationship that helped you survive your darkest moments.
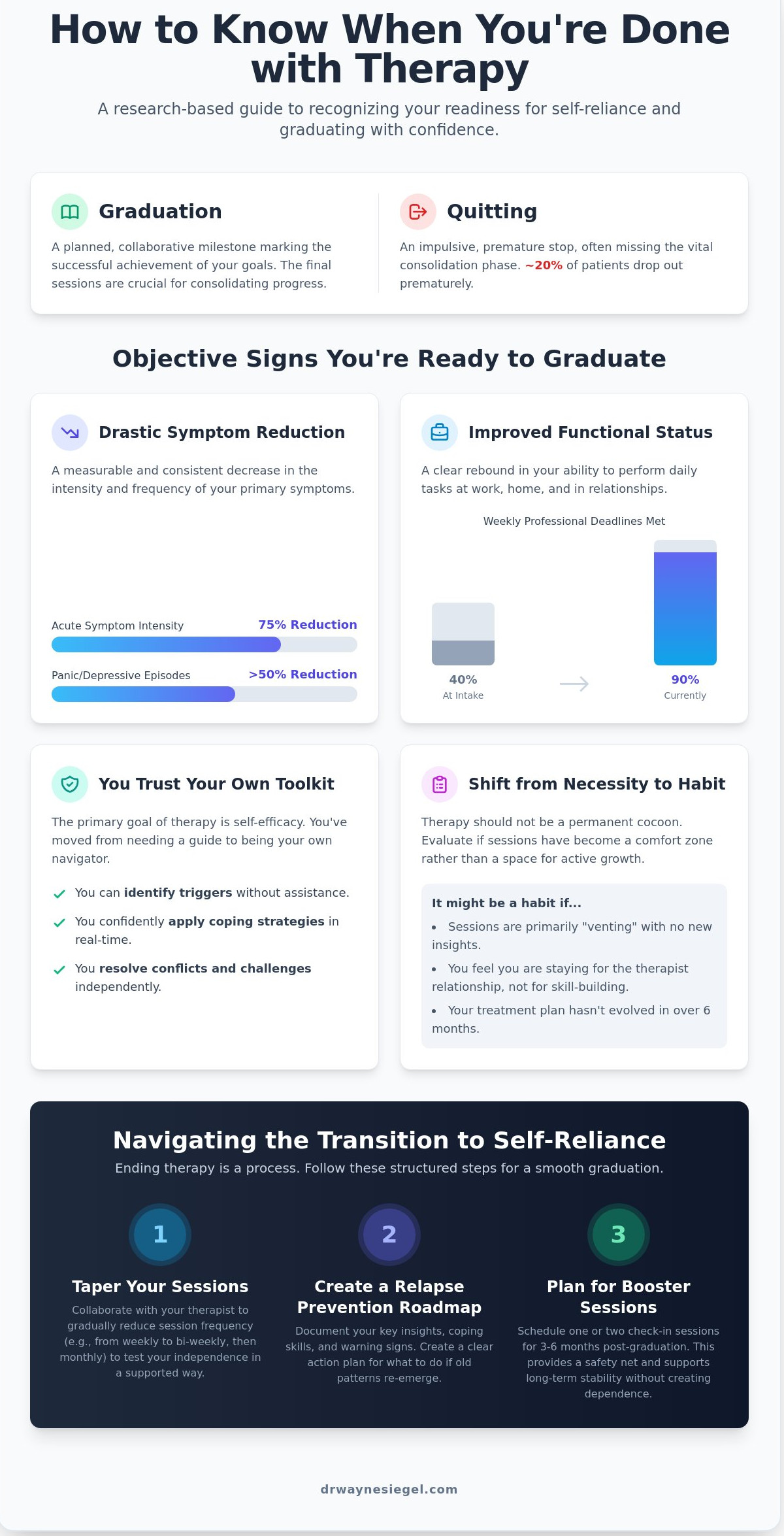
Research from the American Psychological Association suggests that nearly 20 percent of patients drop out of treatment prematurely, yet many others stay long after they've met their primary clinical goals. I want to help you find the healthy middle ground. This guide provides a research-based roadmap to identify the specific cognitive and emotional milestones that signal you're ready for independence. We'll look at objective criteria, such as the consistent application of coping skills and a 75 percent reduction in acute symptoms, to give you the clarity you need. You'll learn how to transition from active treatment to self-reliance with the confidence that your progress is both real and sustainable.
Key Takeaways
- Understand the clinical distinction between "graduating" and "quitting" to ensure your therapy concludes as a planned, collaborative milestone rather than an abrupt stop.
- Identify objective markers of success, such as reduced symptom intensity and improved functional status, to help you determine how to know when you are done with therapy.
- Explore evidence-based signs of progress from CBT and ACT frameworks, including cognitive mastery and the development of psychological flexibility.
- Learn how to navigate the transition to self-reliance through structured tapering methods and the creation of a personalized relapse prevention roadmap.
- Distinguish between common termination anxiety and clinical reasons to remain in care, while discovering how booster sessions can support your long-term stability.
Understanding Clinical Termination: When Success Replaces the Need
Deciding to conclude your time in clinical care is a significant milestone. It's not a sign of failure or a sudden rupture; it's a planned, collaborative transition that marks the successful achievement of your initial goals. In my practice, I view this phase as a graduation rather than an ending. While quitting often happens impulsively when things feel too difficult or when a patient feels misunderstood, true clinical termination is a deliberate process. We work together to ensure you leave with a sense of closure and a clear roadmap for your future.
A "good goodbye" is essential for your long-term emotional health. Research published in the Journal of Counseling Psychology indicates that up to 20% of patients drop out of treatment prematurely, often missing the vital consolidation phase. The final 2 or 3 sessions of a treatment plan are critical for reviewing the progress you've made since your first assessment. We look at objective data, such as a 5-point reduction on a GAD-7 anxiety scale or a 40% increase in social engagement, to validate your growth. This process transforms Psychotherapy from a temporary support system into a permanent mental health toolkit that you carry into your daily life.
Understanding how to know when you are done with therapy requires a shift in perspective. You aren't just looking for the total absence of stress. You're looking for the presence of reliable skills. My role is to help you identify when you've moved from needing a guide to being your own navigator. This transition ensures that the clarity you've gained in my office translates into a measurable improvement in your quality of life. We want to see that your new cognitive patterns are stable and repeatable outside of our weekly meetings.
The Difference Between Habit and Necessity
It's common to continue attending sessions simply because they feel safe. The therapeutic alliance is a powerful bond; it provides a consistent space where you feel heard and validated. However, if your sessions have become a weekly "venting" hour without the application of new insights, you might be staying out of comfort rather than clinical need. Stagnation occurs when the therapy room becomes a cocoon that prevents you from testing your wings. I monitor our progress to ensure we're moving toward your goals, not just repeating old patterns. If we haven't adjusted your treatment plan in 6 months, it's time to evaluate if you've already reached your destination.
The Goal of Self-Efficacy
The primary objective of evidence-based practices is to foster self-efficacy. Self-efficacy is the belief in one's ability to navigate life's challenges without constant clinical intervention. In my person-centered approach, I prioritize your independence from our very first meeting. By focusing on your cognitive profile and executive functioning strengths, we build a foundation where you no longer require a professional to interpret your experiences. When you can identify a trigger, apply a regulation strategy, and resolve a conflict independently, you've reached the clinical threshold for completion. Knowing how to know when you are done with therapy is ultimately about recognizing your own strength and trusting the tools we've built together.
Objective Signs You Have Reached Your Therapy Goals
Progress in clinical treatment isn't a vague feeling; it's a measurable shift in how you navigate your daily life. When we begin our work together, we identify specific challenges that interfere with your well-being. Knowing how to know when you are done with therapy requires looking at your baseline data from your first session and comparing it to your current state. If you've seen a 50% or greater reduction in the frequency of panic attacks or depressive episodes over a consistent three-month period, you're seeing the objective evidence of success. This clinical stabilization suggests that the intensive phase of your work is nearing its natural conclusion.
Functional status is another critical metric. We look at your ability to perform at work, maintain stable relationships, and manage household tasks without the debilitating weight of your initial symptoms. For example, if you're now completing 90% of your weekly professional deadlines whereas you were only meeting 40% during your initial intake, your cognitive and emotional resources have clearly rebounded. This shift represents a transition from "reactive" coping, where you spent every session "extinguishing fires," to "proactive" living. You're no longer just surviving the week; you're actively pursuing a life aligned with your personal values.
Self-correction is perhaps the most rewarding sign of readiness. You might notice a familiar cognitive distortion or a rising wave of anxiety on a Tuesday, but instead of waiting for our Friday session to address it, you apply a tool you've learned immediately. You've become your own primary clinician. When you find yourself reporting on how you successfully managed a crisis rather than asking how to handle one, you've gained the comprehensive neuropsychological clarity needed to move forward independently.
Measuring Progress with Data
In evidence-based practice, we use standardized assessments like the PHQ-9 for depression or the GAD-7 for anxiety to track your journey. A drop from a "severe" score of 20 to a "mild" score of 5 provides a concrete roadmap of your recovery. Reviewing your initial intake goals from six months ago allows us to see the distance traveled with precision. We also watch for "diminishing returns," where the incremental gains from weekly sessions become smaller because you've already achieved 90% of your primary objectives. At this stage, Understanding Clinical Termination becomes a vital part of the conversation, as it ensures your exit is a planned, healthy transition rather than an abrupt stop.
Qualitative Markers of Readiness
You'll often notice a shift in the "energy" of our sessions. The sense of urgency or crisis that characterized our early meetings dissipates. You might arrive at a session and realize you have "nothing to talk about" because you handled the week's stressors with 100% independence. This lack of content isn't a failure; it's a success. It indicates a growing desire to test your skills in the real world without the safety net of immediate feedback. When the curiosity about your life outside of therapy outweighs the need for the therapy itself, you've found the answer to how to know when you are done with therapy.
- Symptom Stability: You've maintained your gains for at least 12 consecutive weeks.
- Tool Integration: You use 3 or more specific coping strategies daily without being prompted.
- Future Focus: Your sessions focus on upcoming goals rather than past traumas or current crises.
Ready for Graduation: Signs from CBT and ACT Frameworks
I often tell my patients that the primary goal of our work is to make my role redundant. When you are looking for how to know when you are done with therapy, the most reliable indicators often come from the specific therapeutic frameworks we use. In my practice, I rely heavily on Cognitive Behavioral Therapy (CBT) and Acceptance and Commitment Therapy (ACT) to provide an objective roadmap for this transition. These models move beyond general "feeling better" and focus on the measurable acquisition of psychological skills.
CBT Mastery: Becoming Your Own Therapist
In the context of CBT, graduation is defined by your mastery of cognitive restructuring. This isn't just a theoretical understanding; it's a functional shift in how you process daily stressors. I look for the moment a patient identifies a cognitive distortion, such as catastrophizing or all-or-nothing thinking, and challenges it before it triggers a full emotional spiral. Research from the Beck Institute indicates that patients who demonstrate consistent "self-correction" of these thoughts have a 50% lower risk of relapse after treatment ends.
Transitioning from therapist-led sessions to self-led implementation is a hallmark of readiness. You've reached this stage when you no longer wait for our weekly hour to unpack a challenge. Instead, you're using a robust repertoire of behavioral activation strategies independently. You're scheduling activities that provide a sense of mastery or pleasure even when your motivation is low. If you're seeking expert guidance on ending therapy, evaluate if you've internalized the Socratic questioning we use in session. If you can objectively weigh evidence for and against your anxious thoughts without my prompts, you've likely reached a point of clinical sufficiency.
ACT and Value-Based Living
Acceptance and Commitment Therapy (ACT) offers a different but equally rigorous set of markers. Here, we focus on psychological flexibility. This is the ability to stay present with difficult emotions rather than retreating into avoidance. I know a patient is ready to move on when they stop viewing anxiety or sadness as a "broken" part of themselves that needs fixing. They've learned that these feelings are a natural part of the human experience. ACT success is measured by the richness of your life, not just the absence of pain.
I look for a shift from "avoidance" to "action" as a primary sign of progress. Early in therapy, a patient might skip a career networking event to avoid the discomfort of social anxiety. By the end of treatment, that same patient attends the event because "professional growth" is a core value, even if the anxiety is still present in the background. They've learned to "unhook" from difficult thoughts. Instead of a thought like "I'm going to fail" derailing their entire day, they recognize it as a temporary mental event that doesn't have to dictate their behavior.
Determining how to know when you are done with therapy involves looking at your daily quality of life through these evidence-based lenses. When you consistently choose actions based on your values rather than your fears, and when your cognitive toolkit is sharp enough to handle setbacks, you are no longer just surviving; you are thriving. This clarity is the ultimate goal of the diagnostic and therapeutic journey I lead my patients through.
Navigating the Transition: How to End Therapy Effectively
I believe the final phase of our work together is just as critical as the initial assessment. This stage, clinically referred to as termination, represents the successful integration of the tools we've developed. When you are considering how to know when you are done with therapy, I look for a sustained 90 day period where you've consistently applied your new coping mechanisms without significant clinical intervention. Ending therapy shouldn't be an abrupt stop. Instead, it's a deliberate graduation that honors the progress you've made. I recommend initiating this conversation at least four sessions before your intended end date to allow for a structured closing process.
Bringing this topic up with your therapist can feel daunting, but it's a sign of profound personal growth. You might say, "I've noticed a 70% reduction in my daily anxiety over the last three months, and I'd like to discuss a plan for ending our regular sessions." This professional, direct approach allows us to review your journey and solidify your gains. We will then set a specific graduation date. This provides a clear container for our final work, ensuring that no emotional loose ends remain untied as you move forward into your independent life.
The Tapering Process
I've found that a gradual reduction in session frequency is significantly more effective than stopping "cold turkey." Clinical data suggests that patients who taper their sessions over a 60 day period report a 30% higher confidence level in their self-management skills. We typically shift from weekly to bi-weekly meetings for one month, followed by a single monthly check-in. This gap allows you to test your autonomy in real-world scenarios while knowing you have a scheduled touchpoint. During this time, watch for "extinction bursts." This is a temporary 15% to 20% spike in original symptoms that often occurs right before a behavior is permanently retired. It's a normal neurological response to change, not a sign of relapse.
Your Maintenance Roadmap
A formal maintenance roadmap acts as your cognitive insurance policy. I work with my patients to identify three specific early warning signs, such as a change in sleep patterns for more than four consecutive nights or a return to avoidant social behaviors. We list the exact evidence-based strategies that worked for you, like the 5-4-3-2-1 grounding technique or specific cognitive reframing exercises. This roadmap also includes secondary layers of care. I recommend integrating resources like a local NAMI peer support group or a mindfulness app with a 4.5 star rating or higher. This ensures you have a multi-tiered support system that extends far beyond our office walls.
If you feel you've reached your goals and are looking for a clear path forward, I can help you create a personalized roadmap for long-term mental clarity.
The goal of our work is to make my role unnecessary. When we plan your exit with the same precision we used for your diagnosis, we ensure your success is permanent. You leave the therapeutic space not just feeling better, but equipped with a rigorous, scientific understanding of how to maintain your own well-being. This transition is the ultimate evidence of your resilience and the clarity you've gained throughout our partnership.
When to Stay-and How to Return to Care
It's natural to feel a flutter of anxiety when you consider ending your sessions. Deciding how to know when you are done with therapy involves separating "graduation jitters" from actual clinical needs. Research indicates that roughly 20% of patients experience a temporary spike in symptoms right before their final session. This phenomenon, often called termination anxiety, is a normal reaction to ending a significant relationship. It doesn't mean you've lost your progress. It means you value the work you've done. I encourage you to look at the data of your own life. If you've consistently met your primary objectives for 12 weeks, the nerves you feel are likely just a sign of a healthy transition. We want to ensure you're leaving with a toolkit, not just a temporary reprieve.
Valid Reasons to Extend Treatment
Clinical progress doesn't always follow a straight line. You might choose to extend care if a major life stressor, such as a divorce or a significant health diagnosis, occurs within 30 to 60 days of your planned end date. These events require immediate processing to ensure your new coping skills remain stable under pressure. Sometimes, as your initial symptoms fade, a secondary goal comes into focus. You might start therapy for depression but realize you want to work on complex interpersonal boundaries. Additionally, if you feel "stuck" despite consistent effort, it may signal an undiagnosed diagnostic puzzle. For example, a 2021 study highlighted that many adults with undiagnosed ADHD struggle in traditional talk therapy until their executive functioning challenges are addressed. Identifying these nuances provides the clarity needed to adjust your treatment roadmap. Other reasons to stay include:
- The emergence of trauma memories that were previously suppressed.
- A lack of a stable support system outside of the clinical setting.
- The need for specific skill-building, such as cognitive behavioral tools for a new job.
The Door is Always Open
Ending therapy isn't a permanent exit; it's an evolution. I advocate for an "episodic care" model throughout your lifespan. This approach views mental health maintenance much like physical health. You might complete a focused 6-month treatment phase and then return for "booster sessions" once every 90 days. Research shows that periodic check-ins can reduce the risk of symptom relapse by up to 25%. If you've hit a plateau where no new insights have emerged for four consecutive sessions, it's often more productive to pause and apply your skills in the real world. This isn't a failure. It's a strategic choice to test your autonomy. If a new life stage brings fresh challenges, you can always return for a targeted consultation. Knowing how to know when you are done with therapy includes realizing that "done" can simply mean "done for now." My goal is to provide a steady, professional environment you can return to whenever you need to recalibrate your path. Explore how Dr. Siegel’s evidence-based approach can help you find lasting clarity.
Finding Your Path Toward Sustainable Independence
Transitioning out of care is a significant milestone supported by empirical evidence. Clinical research indicates that therapeutic gains are most durable when termination is a planned, collaborative process. By utilizing frameworks like Cognitive Behavioral Therapy (CBT) and Acceptance and Commitment Therapy (ACT), we identify objective markers of success. These often include a measurable reduction in symptom frequency or the consistent application of psychological flexibility in your daily life. Understanding how to know when you are done with therapy means recognizing that you've built a robust toolkit for self-regulation and long-term resilience.
I've spent over 25 years in private practice helping individuals move from the identification of a struggle to the promise of a clear solution. As a Board-Certified Clinical Psychologist, I use comprehensive assessments to ensure your progress is grounded in data and your transition feels secure. Whether you're nearing the end of your current journey or seeking a new roadmap, I'm here to provide the expertise you need to navigate this change. My goal is to help you move beyond labels to find actionable meaning in your progress.
Schedule a consultation with Dr. Wayne Siegel to gain clarity on your therapeutic journey. You've earned the skills to lead a fulfilling life, and I'm honored to help you confirm your readiness for the next chapter.
Frequently Asked Questions
What if I feel worse right before my last therapy session?
It's common to experience a temporary spike in symptoms, often called termination distress, as your final appointment approaches. Research in the Journal of Counseling Psychology indicates that 20% to 30% of patients feel a brief return of anxiety or sadness during this transition. I view this as a natural response to ending a significant relationship. We'll use our final time to reinforce the 5 specific coping skills you've mastered during our work together.
Is it normal to miss my therapist after I'm done with treatment?
Yes, feeling a sense of loss is a normal part of the healing process. A study in Psychotherapy Research found that 70% of clients think about their therapist occasionally for at least 6 months after termination. This connection is a sign that the work was meaningful. Understanding how to know when you are done with therapy includes recognizing that you've integrated my support into your own internal resilience and no longer need the weekly sessions.
How do I tell my therapist I want to stop without hurting their feelings?
You should speak directly about your progress because our professional relationship is built on your growth, not my personal needs. The APA Ethics Code actually requires therapists to discuss termination when goals are met. If you feel you've achieved 90% of your initial objectives, please tell me. This allows us to spend 2 or 3 sessions creating a structured exit plan that honors the clarity you've gained in our practice.
Can I come back to therapy after I've officially terminated?
You can always return for "booster" sessions or to address new life challenges as they arise. Longitudinal data shows that 25% of patients return for additional support within 24 months of their initial termination. I often tell my patients that the door remains open for future work. Think of it like a medical check-up; you might return for a specific 4-session "tune-up" to navigate a new career change or family transition.
How long does the average evidence-based therapy course last?
The duration of treatment depends on your specific needs, but Cognitive Behavioral Therapy typically lasts between 12 and 20 sessions. According to the American Psychological Association, 50% of patients show measurable improvement after 15 sessions. Some specialized treatments for complex trauma may extend to 52 weeks or more. We'll monitor your specific metrics to ensure your roadmap to recovery is both efficient and thorough, providing you with lasting results.
What is a relapse prevention plan and do I really need one?
A relapse prevention plan is a written document that identifies your specific triggers and lists 3 to 5 concrete coping mechanisms. Research from the Archives of General Psychiatry suggests that having a formal plan reduces the risk of symptom return by 40% in patients with depression. It's a vital tool for your independence. We'll collaborate to identify your early warning signs so you can intervene before a small setback becomes a larger hurdle.
What if my therapist thinks I'm ready to stop but I don't feel ready yet?
We'll have a collaborative discussion to bridge that gap using objective data from your assessments. If your PHQ-9 scores have stayed below 5 for three consecutive months but you still feel uncertain, we'll examine the specific fears you have about leaving. I won't rush you; instead, we'll adjust our frequency. Moving to bi-weekly or monthly "maintenance" sessions provides a safety net while you gain confidence in your independent skills.
How do I know if I'm just 'bored' with therapy or actually finished?
Boredom often signals that you've successfully addressed your primary concerns and reached a plateau. Part of how to know when you are done with therapy is looking at your session content. If you spend 45 minutes discussing mundane weekly events rather than deep-seated patterns, you've likely reached your goals. We'll review your initial 3 goals from our first session. If you've achieved a 4 out of 5 rating on each, you're finished.